Q: In some northwestern and southeastern states, there is a big push to install stations for HF (long-distance shortwave frequencies) in all the hospitals. Why isn't HDSCS doing that?
A: We have determined that HF stations in our hospitals are not necessary to meet our mission. In all our years of HDSCS support in drills and actual emergencies for dozens of hospitals, we NEVER had an occasion where we needed HF frequencies to handle emergency traffic for a hospital.
We've handled lots of emergency messages. They have all been either unit-to-unit within the hospital, or between the hospitals and community resources such as physicians, utilities, other hospitals, Red Cross, EMS and the like. This traffic is most effectively handled by voice on short-range VHF and UHF frequencies, either via repeaters or simplex. We have never needed long distance HF communication, but if we ever do, we have made plans to pass the traffic out of the hospital on VHF to local home stations that have HF capability. We could also relay the message via the county EOC, where a RACES HF station is located.
Some have claimed that hospitals need to be able to communicate with the state Office of Emergency Services in Sacramento after an earthquake or other wide-area disaster. But the established governmental protocol is quite different. If any Orange County hospital needs additional resources, the first request must go to Orange County Emergency Medical Services Agency. If the county can't provide, a request for resources from the state would be made by the OC-EMS officials. If normal telephone communications are not available, that request would go via RACES from the Orange County EOC, not directly from the hospital. The plan in your area is probably similar, because these are established protocols that are compliant with NIMS (National Incident Management System) and SEMS (Standardized Emergency Management System) policies.
Q: But in our state we have hurricanes that can wipe out communications over many counties, so we need HF stations in our hospitals. Don't you agree?
A: There is nothing wrong with having HF capability at your hospital(s). But don't assume that the installed station, its antenna and its power source will survive the hurricane in operating condition. And please don't delude yourself and the hospital staff into thinking that just because a station is there, the hospital is ready for any disaster. If the hospital doesn't have all of the other important elements of Amateur Radio support (a trained cadre of community hams with portable equipment, an activation plan, liaison with other ARES/RACES/ACS groups, regular drills and so forth), then your HF station may be of little real value and will give a false sense of security.
Q: We have both ARES® and RACES in our county. Which is better for hospital
support?
A: There is a wide variation in policies of ARES and RACES groups around
the country, so there is no hard-and-fast answer to this question. In some
places, ARES and RACES are combined, with members wearing RACES hats during emergency activations
and ARES hats for non-emergency public service communications. In other places
they are separate organizations, with RACES responding to government agencies
and ARES helping non-government entities.
The important thing to consider is that all of your local hospitals must to be
able to get help in isolated emergencies quickly, with no "middlemen." In
widespread emergencies, all hospitals should be checked right away, to verify
that communications have not been disrupted, or if they have, to get help to
them quickly.
A lot of folks tout dual ARES/RACES membership for individual hams and also
combined ARES/RACES groups. Here's what I've seen around the country: When a
combined ARES/RACES group supports hospitals and a disaster occurs, RACES
procedures rule. That means a top-down response, where hams wait for an
official to give them assignments. That mindset assumes that "no news is good news."
You simply can't assume that with hospitals. There's nothing clairvoyant about
county or city officials. How are they going to know that a hospital has a
communications problem if the hospital can't communicate it to them?
That's why we believe that ARES is much more appropriate for supporting private
hospitals than RACES. ARES permits automatic activation (our Core Team response) in widespread disasters such as earthquakes and hurricanes. ARES
also facilitates direct contact from hospitals to hams for quick callout during
isolated (one hospital) phone failures. By comparison, RACES procedures
usually mandate a formal activation by a government official or agency, which
consumes valuable time.
Q: How do we fit hospital support into our existing ARES/RACES organization? Should there be a separate appointed Emergency Coordinator?
A: That depends on the nature of your area and the other
agencies/governments being served by the local hams. Here in Orange County, there is a strong county-level RACES organization and 22
city-level RACES groups. ARES in our county is completely separate from RACES. In recent years, OC ARES primarily has supported the Red Cross and hospitals, although
there are other ARES members-at-large who have been available to support cities and
industries at the non-government level.
I believe strongly that hospitals must
have a priority response at the beginning of any major incident. Patients'
lives and well-being are immediately at risk in any communications failure, and
every hospital is an important resource for the community, especially in
incidents where people have been injured. That's why a specialized ARES
organization (HDSCS) was formed just for hospital support, with its own ARES EC and several
Assistant ECs. It had a separate membership roster, meaning that all
HDSCS members were also ARES members, but not all ARES members were HDSCS members.
In a rural area with only one or two medical facilities and other ARES/RACES
activities such as SKYWARN, it might be OK to have a common roster and to train
every member for a potential response to the hospital. But for any an urban
area where there is a concentration of hospitals, I think a separate ARES
organization such as HDSCS would ultimately be best. Next best would be a
sub-group of ARES members who are dedicated to hospital response and make extra
effort to be involved in hospital drills and meetings. The rest of the ARES
folks would be potential additional responders and should have at least some
education about responding to the hospitals.
Q: Should some of our ARES hams be totally dedicated to hospitals, or could
they also respond to Red Cross and other agencies? Couldn't they also belong
to RACES and ACS?
A: In the mid-1980's, there was a major HAZMAT incident involving 3
cities and the Red Cross in Orange County. When city emergency managers made
calls to activate their RACES radio responders as the incident progressed, they
discovered that the majority of them were already deployed with other
cities or the Red Cross. That soured most of these managers on the idea of
multiple emergency group affiliations and it led to rigid membership
requirements. Many RACES groups in our county now insist that hams that are on
their rosters cannot be members of any other ARES/RACES organization.
By contrast, HDSCS has not insisted on exclusive membership. Since about 80% of
HDSCS activations involved only one hospital and were not widespread incidents, we
weren't about to tell a ham who belongs to Red Cross or a city RACES group that
we didn't want him or her in HDSCS. But we did inquire about the other emergency
group memberships and obligations of our members, and we took that into account
in our planning. We asked new members to declare their group of "primary
allegiance" in responding to a multi-agency or area-wide disaster.
Members who declared HDSCS as their primary response were placed on specific
call-up lists for one or more of our hospitals. In addition to responding
first to HDSCS callouts, these primary responders also identified a hospital that
they live or work close to as their Core Hospital. In a major disaster,
area-wide power failure or phone outage, these hams automatically deployed to
check on their Core facilities, without waiting for a phone call. If they were
somewhere else in the county or nearby in another county when a major disaster
strikes, they came up on our designated frequency, indicated their locations and
availability. Net Control then directed them based on the needs at that time. If Core Team responders were not needed and another agency could use additional
support, we released them.
Hams declaring another group as primary were considered as only general
"Call-up" members of HDSCS. In a multi-agency incident, they were asked to
notify HDSCS if their primary groups do not activate or when they are no longer
needed by that group. This worked very well, because HDSCS was often active
sooner and longer than the other groups. We've gotten relief operators
following earthquakes after some cities deactivated their EOCs.
We haven't let our members cop out and say, "I'll go out with whichever emergency
group calls me first." That ambulance-chaser mentality pits one ham group
against another when disaster strikes. It leaves group leaders wondering how
many potential responders they really have.
Q: Our ARES members are taking the ARRL Emergency Communications Course. What other education do they need to be ready to support hospitals?
A: We've always been pretty good as hams in terms of the communications
and message training that we do. But my observation is that hams aren't
spending enough time to learn about the agencies they support, the procedures
that agencies use on a day-to-day basis, some of the language and the nuances. I'm not expecting hams go out and take a medical terminology course. But if
you're going to be supporting hospitals, it would be good to know a few terms
like "stat," "Code Blue," "Code Red" and the triage terminology. Do you know
what HICS is? You're not going to be an intelligent intermediary for handling
messages in an emergency if you don't get familiar with the hospital and its
most important communications needs.
Learn to match in appearance and attitude. When you go into a hospital, you're
going into a very professional environment. You have to fit in with that if
you want to be taken seriously. You don't need to wear greens or even a
uniform, but you won't be welcome in grubby clothes.
When you talk to hospitals and train your group members, emphasize both
internal and external communications support. The hospital's business-band
walkie-talkies help with internal (unit to unit) messages. Cell phones can
do external calls (from hospital to outside doctor, for instance). However,
ham radio can do both, which is a major advantage.
It's very important to participate in the hospitals' drills. And your
participation needs to be realistic. It's no good for hams to come in an hour
ahead, set up equipment in the lobby, independently transmit a few ham-created
messages to the EOC or disaster site, and then go home without participating in a
critique. That's what college students call "dry labbing," and it hurts our
cause more than it helps.
Make the hospital folks test their activation procedures as part of the drill,
so they will get used to the idea of calling hams right away when
communications fail. It's frustrating to delay the start of hams' drill
participation while waiting for that call, but if you don't do it, the hospital
will get the impression that somehow hams will have ESP and show up without
being called when a backhoe cuts their trunk lines.
Practice some message-handling with the staff. Don't expect that everything in
the drill is going to be wonderful and you're going to get all kinds of good
messages. You have to take them by the hand sometimes. Let them know to whom
you can communicate and suggest a simulated message. Encourage some
third-party interaction, where they talk directly to their counterparts at
other facilities on ham radio.
Participate in the hospitals' critiques after the drills and be an active
listener. You may find an opportunity to explain how ham radio could be of
more assistance.
HDSCS has done a lot of "standby operations," coming in during the wee hours when
new hospital phone or electrical systems are cut in, and so forth. It gave us
good experience and sometimes these operations have turned into real
communications emergencies when things have gone wrong.
Q: Our small ARES group already supports Red Cross and some other agencies. We can't support our hospitals now because we just don't have the people.
A: Maybe you and your emergency group need to take a look at your
priorities. Every hospital is a vital organ in the community. If it needs
help in a disaster and it has no communications to the outside, lives could be
lost. What could be higher priority for ARES communications than that?
Not every potential emergency involves all the other agencies your group
serves. A single-hospital switchboard failure isn't going to require response
by Red Cross.
If you need more members to add hospital support to your ARES activities, get
busy recruiting and training them. On the other hand, if you tell a hospital
official, "We don't have enough people to support your hospital," you may never
get another chance with that facility.
Q: We're planning on having a special licensing class just for hospital
employees. Isn't that best for having radio operators who know the
hospital?
A: Across the country as I talk to hams and emergency groups, I observe
this mindset far too often. A little critical thinking will show that basing
your hospital support plan only on licensed hospital employees is a bad idea.
First, there are legal issues to consider. FCC regulations prohibit hams from
communicating on their bands on behalf of their employers and from accepting
compensation (including wages/salaries) for communicating on ham radio
frequencies for anyone. (FCC 97.113) Spend some time with ARRL's FCC Rule
Book to make sure you fully understand all the ramifications of these
provisions.
There are practical issues also. Let's say that two doctors, a pharmacist
and a biomedical specialist get their ham tickets. What happens to them in a
mass-casualty incident or another disaster when patients descend on the
hospital and communications are overloaded? They'll have to be hard at work at
their regular jobs, of course. They won't be able to provide backup
communications.
In an emergency when phones fail or are overloaded, hospitals need dedicated
communicators. By that I mean listening as well as transmitting. We all get
caught up in being ready to transmit an important message, so we forget that
one of our most important values is our ability to be able to receive important
information, too. If you're a hospital employee, busy with your hospital
tasks, perhaps you can stop to jump on the radio and ask for something you
need. But what if somebody needs something from you? You're not listening,
because you're busy doing your hospital tasks. So you need non-hospital people
as part of hospital communications backup support, because you can't wear all
of those hats.
On average, we've needed 11 hams for each of our emergency callouts, including
a Net Control, base station, and operators in the medical facility or
facilities. Having a few hospital employees would be far from enough. It is
far better to have a cadre of outside volunteer hams at the ready, as we do, to
go into the hospital and perform communication tasks while the hospital folks
go about their emergency medical duties.
Hospital-employed hams can serve as valuable liaisons, but they can't do the
job by themselves.
Q: The hospitals' drills and meetings are usually during the day on
weekdays. That's hard for those of us who work.
A: Weekday hospital drills and meetings are a fact of life. If hams
keep whining about this, hospitals will never believe that Amateur Radio is a
credible, reliable resource. I hear this excuse a lot from hams in other
areas, and it really annoys me because these same hams are quite willing to
take time off from work for the fun parts of our hobby. Remember last Field
Day? How many local hams took the Friday before to prepare and maybe even the
Monday after to recuperate? Same for the hamfests and other contests.
I know that one of the reasons HDSCS was so well accepted in Orange County
is the fact that hams were represented at the major meetings with hospitals. They
also participatde in all the drills, regardless of day of the week or time that they occur. The hospitals trusted
we would be there, and we were.
Q: Our ARES group has an agreement to support the hospital in a disaster. But the hospital's new Disaster Coordinator doesn't seem to know anything about
it.
A: That's the real world. There's a much high turnover rate in hospital
personnel these days. We hams must be willing to continuously re-explain and
re-educate.
When was the last time your ARES EC made contact with the disaster planners at
all of the local hospitals? When was the last time your ARES group participated in a
hospital drill?
Be willing to review your role over and over again with the hospitals. You
simply can't assume that all your local hospital people know and remember all
that we can do. And who knows what kind of internal training they do? I can
educate a Disaster/Safety coordinator over and over, but how much does he or
she pass on to the rest of the hospital staff? So be willing to teach it and
review it with multiple people, every year, multiple times per year. And make
sure that the ham communicators are prepared to educate as necessary every time
they respond.
Offer to teach. I have attended many Disaster/Safety committees, Head Nurse meetings
and hospital in-services to explain Amateur Radio. And ask to be taught,
too. Invite hospital people to your ham group's meetings.
to you how the Laboratory works. Have them tell about Radiology, the burn
center, and so forth.
It's unfortunate, but from what I've seen, far too many hams don't have good
staying power in public service. We want to be EC for a year or two, help the hospitals for a
year or two, and then get out. I understand that it's your hobby, but if
you're serious about helping hospitals, you need to develop regular contacts,
regular participation, and they need to see you regularly. I have gone to about two dozen
hospital disaster and drill planning meetings every year. I also have had
Assistant Coordinators who attended some meetings. When the hospital folks didn't
see me, they usually saw somebody else they knew.
Q: The Administrator of our local hospital says he isn't interested in
Amateur Radio help right now. Why bother?
A: Hospitals are very self-sufficient entities. The reality is that
they will get along without us. But they will get along far better with us in
a disaster, if they understand how to use us and we know how to help them.
Sometimes we hams get whiny when a representative from a local hospital says,
"No thanks, we really don't think we need you." But why should we be surprised
at this initial response, if we haven't had a chance to prove ourselves? Hospital folks don't intuitively understand and envision our capabilities.
And then we hams tend to make things worse because we don't go ahead and
prepare anyway. Since when does a hospital saying it doesn't want you now mean
that it won't ever really need you? Yes, it's true that some hospital
Administrators aren't willing to take a chance on hams. But does that mean
hams shouldn't be preparing to support them in the next big disaster anyway? We're not doing our emergency services for the benefit of those Administrators. We're doing it for the ultimate benefit of patients in the hospital beds. Be
prepared, so you'll be ready in case you're invited in later, or a major
emergency forces the issue.
 Q: It must take lots of money support all those hospitals. What kind of
budget did HDSCS have?
Q: It must take lots of money support all those hospitals. What kind of
budget did HDSCS have?
A: Zero! We had no dues and no treasury. We didn't accept cash gifts and we liked it that way. We've seen far too many other ham
groups getting bogged down in fiscal matters, creating dissention that detracts
from the mission of the group.
Yes, we have had expenses, like this Web site, that have been paid out of members' pockets
or donated by friends of the group. Our supported hospitals have been quite
willing to help us with other needs, in gratitude for our past support to them.
Perhaps you have heard the expression, "No money, no mission." We don't
believe that it's always true. We've learned that you don't need lots of money
to provide Amateur Radio support to hospitals. You just need committed
volunteers.
Q: Could you please provide the HDSCS manuals as a guide for our own group?
A: Because they include specific details about Orange County hospitals and other sensitive information, our HDSCS member manual, other member documents and training materials aren't available to non-members. As a guide to planning support for hospitals in your area, here is a list of topics included in these documents:
- Activation (call up and pager) procedures for single hospital phone outages and mass casualty incidents
- Instructions for automatic (Core Team) response in area-wide Disasters (e.g. earthquakes)
- Protocols to be followed upon arrival at hospitals
- Our repeater/simplex frequencies, their tactical references and other access information
- Equipment preparedness, for go-kits and vehicles
- Personal and home preparedness
- Hospital response groups (EMS color-coded nets)
- Hospital locations, driving directions, and maps
- How hospitals are organized and how they respond in a crisis (e.g. HEICS and EMS System)
- Other hospital communication systems such as HEAR/ReddiNet, county radios, etc.
- Special procedures for HAZMAT incidents
- Message forms and special instructions for medication ordering
- Other in-hospital issues, e.g. appearance, confidentiality, stress, dealing with media
- How HDSCS interfaces with EMS, NDMS, NIMS and other agencies/systems
- Frequencies and contact information for other local and nearby ARES/RACES groups
- Glossary of important medical and EMS terminology
In the Photos At top: Almost every large medical facility is expanding, remodeling, or planning to do so. Many California hospitals are rebuilding to meet new stringent earthquake standards. Every time a hospital "cuts in" a new phone system or interrupts utilities for some other construction-related reason, there is an opportunity for a "standby operation," where hams provide backup communications during the changeover. In center: HDSCS member Roman Kamienski KG6QMZ helps install an Amateur Radio VHF/UHF antenna atop an Orange County hospital. Near bottom: Bob McCord K6IWA operates ham radio gear in the Orange County EMS command vehicle. The HDSCS mission has expanded in recent years to include support to the Orange County Healthcare Agency and EMS.
*Formerly the Joint Commission for the Accreditation of Hospitals (JCAH, 1951) and the Joint Commission for the Accreditation of Healthcare Organizations (JCAHO, 1987)

Back to the HDSCS home page
This page updated 14 October 2018
 A: Here's a case where it usually isn't best to go to at the top. Except in very small facilities, the CEO and Administrator usually delegate
disaster preparedness tasks to others. In most cases, you should start with
the Disaster/Safety Coordinator. Only very large hospitals have a
Disaster/Safety Coordinator who does nothing else. Usually the position is
shared by the Telecommunications Manager, Emergency Department nurse, or
Director of Engineering/Facilities. The administrator may need to approve any
ham radio participation at the hospital, but it's best if the hospital's Disaster
Coordinator initiates this.
A: Here's a case where it usually isn't best to go to at the top. Except in very small facilities, the CEO and Administrator usually delegate
disaster preparedness tasks to others. In most cases, you should start with
the Disaster/Safety Coordinator. Only very large hospitals have a
Disaster/Safety Coordinator who does nothing else. Usually the position is
shared by the Telecommunications Manager, Emergency Department nurse, or
Director of Engineering/Facilities. The administrator may need to approve any
ham radio participation at the hospital, but it's best if the hospital's Disaster
Coordinator initiates this.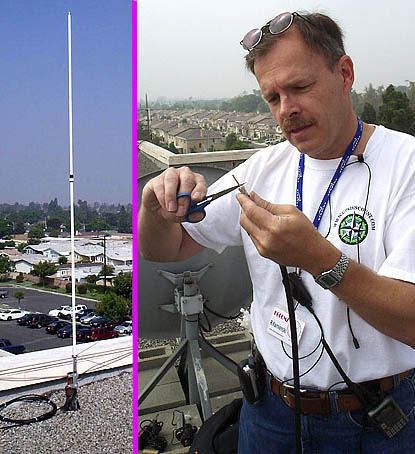 A: All we have asked is for each hospital to install is one or more rooftop VHF/UHF
antennas for our county-wide communications, with coax cable going to key areas
such as the Hospital Command Center and PBX. Because we use
three VHF/UHF bands, we prefer multi-band antennas such as the Comet CX-333
2m/125cm/70cm tribander. Many times the coax
run must be over 100 feet, so we recommend Times LMR-400 or similar low-loss
cable.
A: All we have asked is for each hospital to install is one or more rooftop VHF/UHF
antennas for our county-wide communications, with coax cable going to key areas
such as the Hospital Command Center and PBX. Because we use
three VHF/UHF bands, we prefer multi-band antennas such as the Comet CX-333
2m/125cm/70cm tribander. Many times the coax
run must be over 100 feet, so we recommend Times LMR-400 or similar low-loss
cable.